The Lockdown Files have dished up a curious exchange among Britain’s top policy advisers in early 2020. On 29 February, responding to a WhatsApp message from Prime Minister Boris Johnson’s chief adviser Dominic Cummings that Israeli scientists were just weeks away from developing a Covid vaccine and if this was credible, Chief Scientist Sir Patrick Vallance replied “Short answer is no.”
Chief Medical Officer Chris Whitty explained: “For a disease with a low (for the sake of argument 1%) mortality a vaccine has to be very safe so the safety studies can’t be shortcut. So important for the long run.” England’s highest mortality rate was in April 2020 at 0.6 percent, falling to 0.55 percent in January 2021 and 0.04 percent by January 2023.
Based on the original Phase 3 trial data, Bart Classen showed as early as August 2021: “Results prove that none of the vaccines provide a health benefit and all pivotal trials show a statically significant increase in ‘all cause severe morbidity’ in the vaccinated group compared to the placebo group.”
This is nicely book-ended by a recent (16 March) CDC report showing US maternal mortality jumped to 1,205 in 2021 compared with 861 in 2020 and 754 in 2019.
The 2021 rate of 32.9 maternal deaths per 100,000 live births is the highest maternal mortality rate since 1965. Hmmm, let’s see. What was the newly introduced pharmaceutical intervention in 2021 that begins with “v,” that must not be named in connection with unexplained deaths. that also exacerbated the damage to healthcare access caused by the nonpharmaceutical interventions?
As Sonia Elijah comments, drug regulators withdrew 20 common cough and cold remedies earlier this month “because of concerns about a ‘very rare’ risk of anaphylaxis.” The European Medicines Agency identified anaphylaxis as an important risk from Pfizer’s Covid-19 vaccine way back when in December 2020 and flagged it again in August 2021.
So the vaccine was withdrawn immediately, you ask? I like your sense of humour. And please do try to remember that anyone dying within 14 days of a Covid injection was in reality “unvaccinated.”
Thomas Buckley summarizes it succinctly:
Tetanus boosters are not scheduled every four months … and polio is an awful memory of the past.
Covid is still around and, most likely, will be forever, as will the growing list of health problems associated with the shot itself….
From two weeks to stop the spread to get a not-vaccine shot every four months, the pandemic response has been full of lies and suffering for the general public and money and power for the autocrats and oligarchs and their clerisy.
The malfeasance was compounded by the cowardice of political leaders hiding behind “Follow The Science” that mistook a slogan for policy and let loose upon democratic societies previously unimaginable acts and scenes of censorship, coercion and brutality that has eroded trust in authorities and institutions.
Sadly, regulators have become vaccine enablers first, more committed to defend vaccines from criticism than protect people from harmful vaccines.
Setbacks to The Narrative
Panic saw 100 years of evidence-based pandemic response programs junked. The accumulated wisdom was to quarantine the sick, not those feeling well; to prioritize the most vulnerable, not coerce the least vulnerable. I’ve gone back to read the CDC’s 2017 “Community Mitigation Guidelines to Prevent Pandemic Influenza.” Among its conclusions:
- The CDC “might recommend the use of face masks by ill persons as a source control measure during severe, very severe, or extreme influenza pandemics when crowded community settings cannot be avoided.” However, “little evidence supports the use of face masks by well persons in community settings.”
- “Persons in community settings who show symptoms consistent with influenza and who might be infected with (probable) pandemic influenza should be separated from well persons as soon as practical, be sent home, and practice voluntary home isolation.”
While Sweden was a lonely outlier in sticking with existing science and plans, almost all others chose experimentation over decades of experience. Bizarrely, with lockdown normalized as the default response, Sweden was the one called on to explain staying with its existing plan.
This happened because superstition-driven diktat took over in the wish to be seen to be doing something. Fear was instrumentalized to terrify citizens. A Yale study in November 2021 concluded that public health messaging was effective in shaming and embarrassing people into getting vaccinated to protect themselves, in the belief that this would also expedite the date on which the entire community could be released from the restrictions.
Focussing on Only One of Three Metrics
Yet vaccines were tested for reducing the likelihood of infection leading to serious illness and death, not for protecting against infection and transmission. Robert Blumen has noted how manufacturers and health authorities ignored the more troublesome numbers of absolute risk reduction and numbers needed to vaccinate. Instead, they concentrated in weaponising the relative risk reduction of 95 per cent so that people were misled into believing it meant 95 percent protection against infection, rather than a 95 percent reduction in the risk of those infected to progress to severe disease: “Covid injections were a treatment, not a vaccine.”
There would never have been the widespread public backing for vaxports if people had not been misled into exaggerating the threat from Covid by several factorfold and mistaking relative for absolute risk reduction. This led them into the false belief that mass vaccination would end the pandemic and the unvaccinated were selfishly prolonging that day of release.
The brainwashing was so effective that to this day many insist that the high rate of vaccination protected Novak Djokovic from Covid.
The virus and the disease are two different things that became conflated in the public discourse. “Coronavirus” is a generic term that includes a large family of viruses with spiky projections on their surface that look like crowns. SARS-CoV-2 is a specific virus. Covid is the respiratory illness caused by the virus (just as measles is the disease caused by the virus rubeola).
Anyone could catch the virus, but the health risks from the disease were steeply age-dependent. So yes, the virus doesn’t discriminate, but no, we were not in it together. The conflation of the virus and the disease led directly to the policy confusion that dismissed targeted protection in favour of universal prescriptions.
A Covid vaccination helps the body to build immunity against the disease. A person with enhanced immunity to developing the disease owing to being vaccinated can still carry and transmit the virus that causes the disease.
The three key and distinct numbers for assessing vaccine efficacy are absolute risk reduction, relative risk reduction, and number needed to vaccinate (NNV). The vaccine manufacturers and promoters engaged in a misleading campaign.
A Lancet article gave the relative risk reduction of five vaccines from 67 to 95 percent, but their absolute risk reduction ranged from 0.84 percent for Pfizer to 1.3 percent for AstraZeneca: not so impressive but far more realistic. A 95 percent efficacy within a 1 percent subgroup will barely register as a blip on the mortality curves.
On the number needed to vaccinate, CDC Director Rochelle Walensky tweeted on 25 June 2021 that among 12-17 year olds, one million vaccinated protect one death. To estimate the benefit-harm ratio, therefore, we would need to know the injurious side-effects for that age group.
This is where Aseem Malhotra’s calculations are pertinent. The NNV to prevent one Covid death for 18-29 year olds (figures for the younger cohort are not given) during the Delta variant’s dominance in the three months after vaccination was 93,000. The risk of a serious adverse event (that results in hospitalization or disability) from an mRNA vaccine is 1 in 800. In summary, therefore, Pfizer’s original trial data suggested that there is “a greater risk of serious adverse events from the vaccine than from hospitalisation because of Covid-19.”
The puzzle of why there was a worldwide cascading abandonment of a hundred years of accumulated knowledge by scientific and policy advisers will occupy researchers for many years. The result is that old lessons are having to be relearned. Judging by the rush of studies now coming through to contradict key tenets of the 2020–22 narrative, there’s hope that the wall of silence rooted in groupthink and fear of consequences to career and reputation might have been irreparably breached.
Recent Studies
At the community level, neither isolation nor vaccination but socialization confers the best immunization. A study in the Proceedings of the National Academy of Sciences last July showed that lack of household exposure to kids increased Covid hospitalization of grown-ups by 27 and ICU admission by 49 percent.
The state turned out to be the most efficient Granny killer along with the biggest purveyor of mis- and disinformation. A study of almost 300,00 people in California found that adults have sharply elevated risks of being diagnosed with heart, skin and psychiatric conditions in the three months following Covid injections. In February, three years later, the Lancet published a meta-analysis of 65 studies confirming that immunity conferred by prior infection is real, robust and long-lasting, at least as protective as two doses of the mRNA vaccines.
A study from George Mason University in February found that vaccine mandates in nine US cities did not increase vaccine take-up, undermining one of their key justifications. Data released in February by the Office of National Statistics showed that in England, deaths among the vaccinated was disproportionately higher for all age groups for most of 2021 and 2022. Another study by a Slovenian team, published in preprint, found the mortality of vaccinated-infected groups to be 14.5 percent higher on average than that of non-vaccinated groups.
An earlier study in 2022 found that across 19 European countries, birth rates fell nine months after vaccine rollouts gathered speed. Pfizer began a clinical trial in February 2021 to examine the safety and efficacy of its mRNA vaccine in pregnant women and their newborns but the release of data from the trial is still awaited.
Perhaps the biggest surprise is an article in Cell Host & Microbe published on January 11, 2023, with Anthony Fauci as one of the co-authors. Contrary to the good doctor’s many absolutist claims while still in office, this article concedes that “it is not surprising that none of the predominantly mucosal respiratory viruses have ever been effectively controlled by vaccines.”
Non-sterilizing Covid vaccines could and should never have been expected to significantly reduce infection or transmission. Here is a five minute compilation of Anthony Fauci’s many inconsistencies, contradictions, and denialism.
Dr. Guy Hatchard has drawn attention to two studies by authors from the New Zealand Ministry of Health that show (1) a statistically significant association between Pfizer Covid vaccines and myocarditis and acute kidney injury, (2) correlation between vaccination status and mortality in 2021–23 inclusive, and (3) compared to the 73 percent of those eligible who had received Pfizer booster shots, the boosted account for a disproportionate 80 percent of all Covid deaths.
Other studies show successor doses are less effective and repeated doses may be driving infections. A study in December in Science Immunology by German scientists indicated that the third and subsequent doses of mRNA vaccines could be weakening the immune system, increasing the risk of infection and of prolonging and making the illness more serious.
In the same month, another study of employees of the Cleveland Clinic in Ohio also found, contrary to the authors’ expectations, that infection rates increase incrementally with each successive dose of a Covid vaccine. The triple-vaccinated had infection rates three times higher than the unvaccinated.
A study published in February found that mRNA vaccines contain billions of particles of self-replicating DNA that can turn human cells into permanent factories for Covid-19 spike protein. This could explain the persistence of spike protein and mRNA in the body for months after injection.
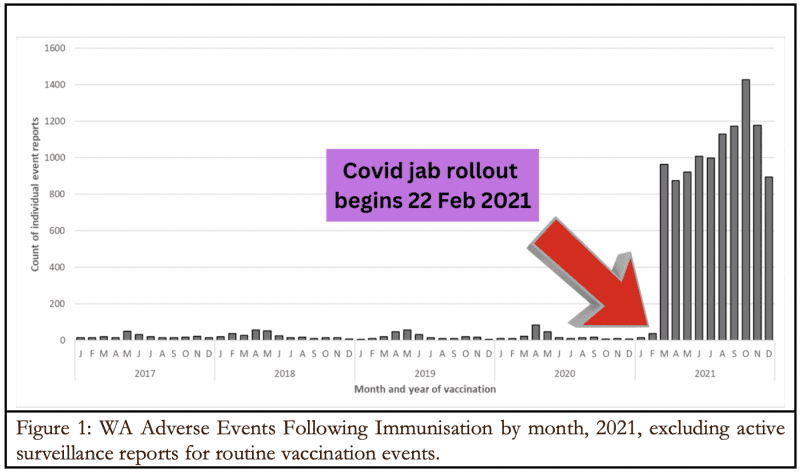
An analysis of the situation in Western Australia is especially interesting, because although 4 million vaccine doses were administered in 2021, border closures to interstate and international travel were zealously enforced to protect the state as an infection-free-zone. Subsequent adverse events therefore cannot be attributed to Covid.
In an analysis posted on 14 March, Rebekah Barnett notes that the rate of adverse events for Covid vaccines (264.1/100,000 doses) was almost 24 times higher than all others (11.1). The number of adverse events in 2021 – remember, there was almost no Covid in WA that year – was 10,726, 39 times higher than the average of 276 per year in the 2017–20 period. She quotes the annual WA Vaccine Surveillance Report:
The number of adverse events following immunisation … was significantly higher in 2021 than in previous years … due to the introduction of the Covid-19 vaccination program.
The impact of the Covid vaccination campaign in 2021 on reported adverse events is visually quite dramatic in her first chart (Figure 1). Some of the key takeaways are:
- Women were disproportionately affected (64 percent);
- Contrary to claims from the national drug regulator, 57 percent of those adversely affected required treatment in the emergency department of hospitals;
- The hardest hit age bracket was the 30–49 year olds;
- Background rates of myocarditis and pericarditis increased by 35 and 25 percent, respectively.
The lockdown harms are showing up in excess death counts, job losses, supply chains chaos and rising costs of living. This may get worse in the next 2-5 years before it begins to normalize. Sweden is an absolute standout in bucking this trend (Figure 2).
I wonder why? Could it be that if we hadn’t shut down the economy and healthcare, cancelled cancer and coronary work, induced mass fear in the general populace, stopped people exercising in the open air and not intensified social isolation by preventing people talking to one another, we might, just possibly might, have had lower excess deaths?
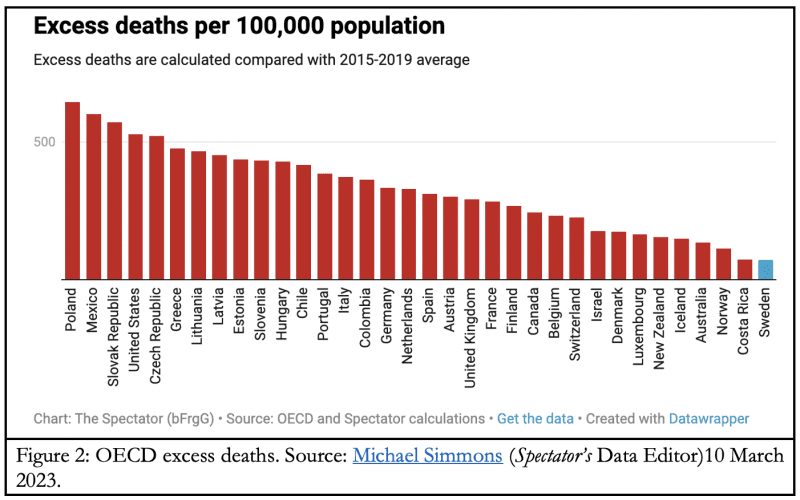
The Lockdown Files show UK Health Secretary Matt Hancock getting increasingly riled by the Swedish counterexample. I am sick of the “fucking Sweden argument,” he said, and demanded “three or four bullet [points] of why Sweden is wrong.” He didn’t inquire if Sweden was wrong. Assuming that, he wanted to be able to show why it was wrong: a perfect example of policy-based evidence.
That said, Sweden’s exceptionally low excess death count is also a strong cautionary note against popular arguments conflating vaccine-excess deaths correlation with causation. Will Jones, editor of The Daily Sceptic, explores several alternative hypotheses on the link between excess deaths, the virus, lockdowns and vaccines.
Conclusion
The vast majority of Covid deaths in many countries by now are among the vaccinated and boosted. This proves conclusively the ineffectiveness of vaccines at the community level, totally discredits the premise of vaccine mandates, but leaves open the possibility of net protective benefits for target groups like the elderly and people with comorbidities.
The policy conclusion is to lift mandates in public settings and prohibit companies from imposing them in most business settings, leaving it instead for people to make informed decisions in consultation with their doctors, without pressure on the latter from drug regulators.
For all the eye-watering amounts of money transferred from taxpayers to Big Pharma, the Covid vaccines would seem mostly to bear little causal relationship to mortality outcomes:
- Not every death listed as a Covid death was caused by Covid;
- Not every vaccinated person who died was killed by the vaccine;
- Not everyone who was vaccinated, infected by the virus and got sick with Covid but didn’t die, lives because of the vaccines;
- Among the unvaccinated also, conversely, not everyone who died from Covid, did so because they avoided the jabfest;
- Not every unvaccinated person who was infected by the virus and got sick with Covid but didn’t die, lives because of avoiding the vaccine.
The important point is the imperative need to investigate the phenomenon. The refusal of governments to do so is exasperating but perhaps also very telling: Never ask a question to which you don’t know the answer.
Lockdowns also locked in generational poverty and inequality in and across nations. Historical illiteracy is now a job requirement for “experts.” Recalling Margaret Thatcher’s comment on the trouble with socialism, politicians don’t learn from mistakes made with other people’s health and money. The media too lived down to their description as stenographers with amnesia. The state dictated every aspect of peoples’ lives, down to the most ridiculous, absurd and intimate details.
With no known cure for blind faith in governments, people embraced compliance with draconian directives from politicians proffering iron fists as a magic bullet.
On every major point of contention in managing the pandemic, the Great Barrington Declaration was right. The common sense distilled into the few words of the Great Barrington Declaration was an uncommon virtue. Fearmongers-in-Chief like Neil Ferguson, Anthony Fauci (whose omniscience deserted him during deposition) and a host of PUIs (Pfizer’s useful idiots) were wrong. The three eminent scientist-authors were taken down savagely and belittled as “fringe epidemiologists.”
From Twitter Files #18 and #19 released by Matt Taibbi, we now know that government agencies, NGOs, academia, Big Tech, media, and the intelligence community colluded in the Virality Project led by Stanford University to censor as mis/disinformation even true stories if their effect was to promote vaccine hesitancy. This included true accounts of vaccine injuries.
As Andrew Lowenthal puts it, rather than highlight safety signals to protect the public, the censorship-industrial complex
ran cover to protect Big Pharma, smearing and censoring critics. The moral depravity is astounding and quite possibly criminal.
This misuse of government power is a genuine threat to democracy, not a confected one.
Join the Conversation
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








